-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(2): 598-603
doi:10.5923/j.ajmms.20261602.45
Received: Nov. 12, 2025; Accepted: Dec. 8, 2025; Published: Feb. 7, 2026

Treatment of Postoperative Radicular Pain Syndrome with Pulsed Radiofrequency Ablation of Spinal Cord Ganglia
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKarim Rakhmatov
Bukhara State Medical Institute, Bukhara, Uzbekistan
Correspondence to: Karim Rakhmatov, Bukhara State Medical Institute, Bukhara, Uzbekistan.
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Radicular syndrome or radiculopathy (radiculitis, radiculoishemia) is a symptom complex resulting from compression or irritation of the spinal roots, which includes pain syndrome in the spine and/or in the extremity (less often in the trunk and internal organs), tension symptoms and deficient neurological symptoms in the dermatome corresponding to the affected root and/or myotoma. In addition to radiculopathy, back and limb pain can occur with numerous myofascial syndromes, dysfunction of the facet and sacroiliac joints, as well as with tunnel neuropathies. To determine the tactics of treatment, the correct diagnosis of the cause of pain in the patient is crucial. Radiculopathy (M54.1) and sciatica (M54.3) have different etiopathogenetic mechanisms of occurrence: in the first case, it is a herniated disc causing a disc-radicular conflict, in the second, tunnel neuropathy of the sciatic nerve caused by spasm of the piriformis muscle. Consequently, in the treatment of radiculopathy, it may be advisable to use surgical methods of root decompression by discectomy, while in the treatment of sciatica, the need for surgical methods of treatment (neurolysis, spicotomy) occurs much less frequently.
Keywords: Degenerative spine conditions, Radicular pain syndrome, Epidural blockade, Pulsed radiofrequency ablation, Failed back surgery syndrome
Cite this paper: Karim Rakhmatov, Treatment of Postoperative Radicular Pain Syndrome with Pulsed Radiofrequency Ablation of Spinal Cord Ganglia, American Journal of Medicine and Medical Sciences, Vol. 16 No. 2, 2026, pp. 598-603. doi: 10.5923/j.ajmms.20261602.45.
1. Introduction
-
Radicular pain syndrome is the main surgical target in the surgery of degenerative spine conditions (DSC). The retention or recommencement of radicular pain after a successful operation without an obvious substrate for re-intervention is the basis of the so-called "failed back surgery syndrome" (FBSS). The frequency of occurrence of FBSS is determined by different authors in the range of 10-40%, depending on the choice of assessment methodology, initial pathology and type of surgery [1]. There are no generally accepted approaches to the treatment of chronic radicular pain after surgery; most non-invasive methods have a weak evidence base and are supported by a limited number of low-level works [2]. Interventional methods show reliably better results, and the ineffectiveness of interventional methods of pain treatment is a criterion for the diagnosis of FBSS and an indication for neuromodulation [3,4], at the present time, 1–2 classes works have confirmed the effectiveness of epidural administration of glucocorticosteroids and percutaneous adhesiolysis [5]. Pulsed radiofrequency (PRF) ablation is a pain treatment method based on the ultrastructural effect of high-frequency current on myelin-free nerve fibers to simulate the passage of a pain impulse. Studies of various levels demonstrate the effectiveness of the method for the treatment of pain syndrome of various etiologies, including radiculopathy. [6], at the same time, the number of works devoted to the treatment of radicular pain after surgical treatment is small, the results are contradictory, in most cases, patients were jointly studied without a history of surgery [7].
The purpose of this study is to evaluate the possibility of using PRF of the spinal ganglia in combination with epidural blockade (EB) for the treatment of radicular pain syndrome after surgical interventions for degenerative-dystrophic diseases of the lumbosacral spine.
2. Materials and Methods
-
This work analyzes a subgroup of patients from the basic study devoted to the diagnosis and treatment of pain syndromes after surgical treatment of DDD of the lumbar spine, which was performed in the period 2017–2019 [8]. Within the framework of the basic study 155 patients were prospectively investigated and traced. The subgroup of patients with postoperative radicular pain syndrome who met the selected eligibility criteria made 28 people. 11 patients of the main group underwent PRF of the spinal ganglia in combination with EB, 17 patients of the control group - only EB by transforaminal approach. For the analysis, we selected patients who were initially or reoperated at one or more levels for spinal disc herniation (SDH) or degenerative spinal stenosis in the volume of discectomy / decompression or decompression with posterior interbody fusion and transpedicular fixation, with radicular pain syndrome [9].
Acceptance criteria.
1. Radicular pain syndrome that persists after the intervention or appears within 1 year after it.
2. Pain level - 4 or more points on the digital pain scale (NRS-11) and / or 8 points or more on the index of anxiety caused by radiculopathy, and / or disability 20% or more on the Oswestry Disability Index (ODI).
3. Absence of obvious compression factors on the basis of postoperative magnetic resonance imaging (MRI) and / or computed tomography (CT), as well as melography in the form of incompletely removed SD hernia or eliminated stenosis, incorrect position of transpedicular screws or migration of an interbody implant. Epidural fibrosis was not considered a compression factor. The presence and degree of root compression was assessed according to the C.S. Pfirrman et al. classification [10], spinal stenosis - according to the classification of C. Schizas et al. [11], foraminal stenosis to the classification of S. Lee et.al., perforation of the medial wall of the root of the arch was allowed and the distance of the screw into the canal was not more than 4 mm, based on the recommendations of the review by E.J. Woo, M.N. DiCuccio [12].
4. No reduction in pain syndrome (at least 50% or 4 points on the NRS-11 scale, 20% ODI, 8 points SBI) while taking at least one drug from the group of antidepressants or anticonvulsants recommended for the treatment of neuropathic pain in adequate dosages in within 1 month [13].
5. With the predominant localization of pain in the lower limb above the knee, pain associated with movement, the presence of chronic back pain, in order to exclude other possible mechanisms of pain syndrome formation, a single test blockade of intervertebral joints and / or sacroiliac joints with a 0.2% ropivacaine solution was performed in a number of patients under fluoroscopic control. When pain syndrome decreased by 50% or more on the NRS-11 scale, patients were excluded from further analysis [14].
The presence of chronic back pain as a leading clinical syndrome, radiculopathy without pain syndrome, extremely severe pain syndrome, severe neurological deficit, signs of an infectious process [15].
The tools for assessing the preoperative state and outcomes of the interventions were the NRS-11 and SBI indices to determine the intensity of pain syndrome and the ODI index to assess the disability [16]. Patient achievement of a positive outcome was the main study outcome of the present study. A positive result was considered a decrease in the NRS-11 index by 50% or by 4 points, and / or a decrease in the ODI index by 20%, and / or a decrease in the SBI index by 8 points from the baseline values with the preservation of the effect for 6 months or more. Patients were examined for a year with control after 6 and 12 months from the date of the procedure [17]. In the presence of the fact of performing other interventional procedures and / or increasing the dose of analgesic drugs, as well as in case of loss of contact with the patient during the first 6 months, the result was considered negative [18]. Key outcomes were assessed by telephone interview, email, or outpatient visit 6 and 12 months after the procedure [19].
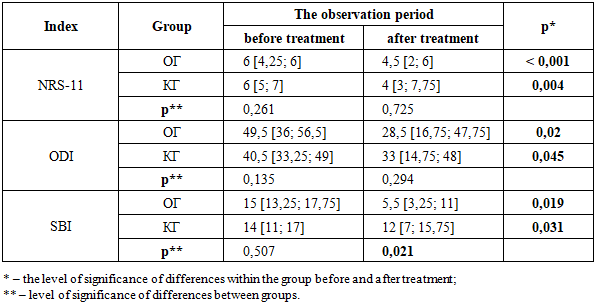
The dynamics of the studied indices NRS-11, ODI and SBI were analyzed before and 6 months after the procedure. To search for factors influencing the positive outcome of interventions, the following indicators were taken into account and analyzed: age, gender, number and volume of surgeries for this pathology in anamnesis, presence of allodynia or hyperpathy, presence of neurological deficit, duration of pain syndrome before intervention, level and number of affected roots [20].
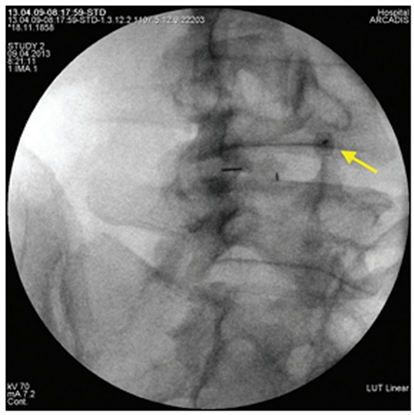
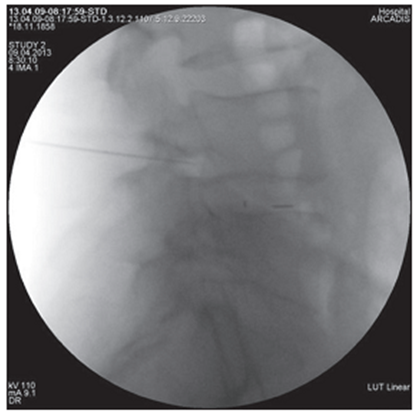
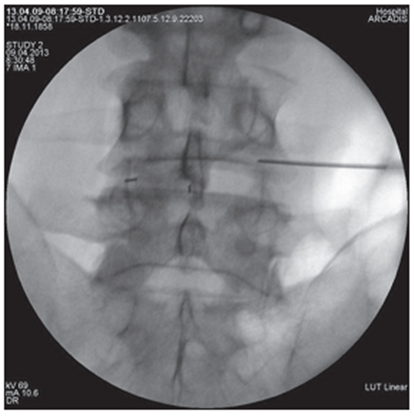
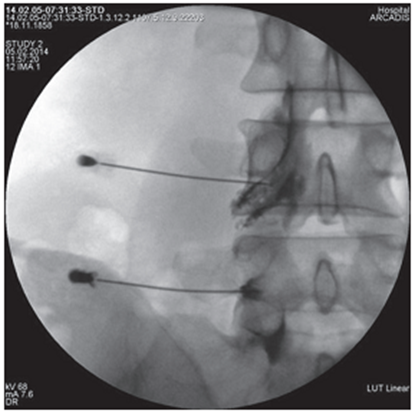
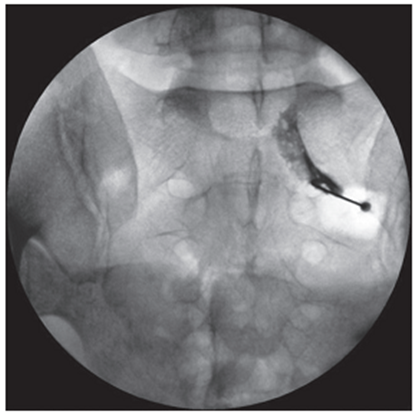
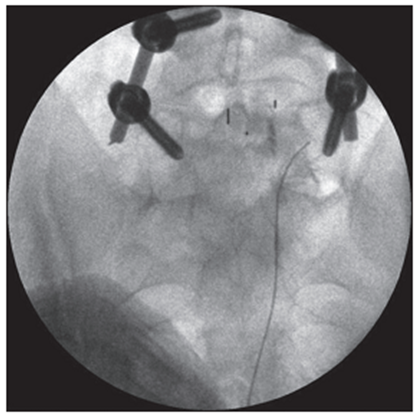
All interventions were performed by one researcher in an operating room equipped with a mobile X-ray machine with a C-arch, in the prone position of the patient under local anesthesia with monitoring of vital functions [21]. Under fluoroscopic control in oblique projection, a puncture needle or an ablation needle was inserted and passed into the area between the apex of the superior articular process of the underlying vertebra and the root of the arch of the overlying vertebra (Fig. 1). In the lateral projection, the tip of the needle should have taken a position in the posterosuperior quadrant of the intervertebral foramen (Fig. 2), in the straight line - no further than the medial pedicular line (Fig. 3). During subsequent epidurography, the spread of contrast was assessed, in the absence of adequate contrasting of the epidural space or with intravascular spread, the position of the needle was changed (Fig. 4). Taking into account the possible features of the distribution of the contrast agent and the drugs administered after the cranial or caudal spread (Fig. 4), in the case of monoradicular syndrome, the transforaminal approach was carried out at two levels - at the pathology level and below, with the biradicular - at three levels [22]. In pathology at the LV-SI level, to isolate the S1 root, the access was performed through the first sacral foramen (Fig. 5), to perform PRF of the spinal ganglion S1 - through the hiatus sacralis using an epidural electrode (Fig. 6), which is associated with the anatomical features of the sacral structure and the technical difficulty of reaching the spinal ganglion through the sacral foramen. In the main group, an ablation electrode was installed in the needle and sensory and motor stimulation was performed with threshold values of 0.5 V and 1.0 V, respectively, for additional verification of positioning near the target nerve, if the indicated stimulation thresholds were exceeded, the position of the needle was corrected [23]. Pulsed radiofrequency ablation was performed for 10 minutes with the following parameters: voltage 65 V, pulse duration 5 ms, frequency 5 Hz, temperature limit 42°C, at the end of the procedure, epidural injection of a total of 5–8 ml of 0.2% ropivacaine solution was carried out through each needle and 1 ml of a suspension containing 40 mg of triamcinolone acetonide. In the control group, only epidural administration of these drugs was carried out [24].
|
Figure 1. Intraoperative X-ray of the lumbar spine in oblique projection. The puncture needle (marked with an arrow) is located in the area between the apex of the superior articular process of the LV and the root of the LIV arch on the right |
|
Figure 2. Lateral intraoperative radiograph of the lumbar spine. The tip of the puncture needle is located in the upper outer quadrant of the intervertebral foramen LIV-V |
|
Figure 3. Lumbar intraoperative radiograph spine in direct projection. The tip of the puncture needle is located in the LIV-V intervertebral foramen on the right along the medial pedicular line |
|
Figure 4. Intraoperative X-ray of the lumbar spine in frontal projection. Epidurography and possible routes of contrast agent distribution |
|
Figure 5. Intraoperative X-ray of the lumbar spine in frontal projection. Puncture of the first sacral foramen and spread of contrast along the root S 1 |
|
Figure 6. Intraoperative X-ray of the lumbar spine in frontal projection. The epidural electrode is inserted through the hiatus sacralis and is located in the projection of the spinal ganglion S 1 on the left |
3. Results
-
Of 155 patients with pain syndromes after surgical treatment of DDD of the lumbar spine, 45 patients (29%) had pain in the lower limb without an obvious compression substrate according to neuroimaging data. When performing test blockades for differential diagnosis in 13 patients (8.4%), pain relief was achieved, against the background of correction of conservative treatment, a positive effect was achieved in 5 patients (3.2%), as a result, 56 patients underwent interventional interventions, all they are traced for a year after the procedure and included in the final analysis.
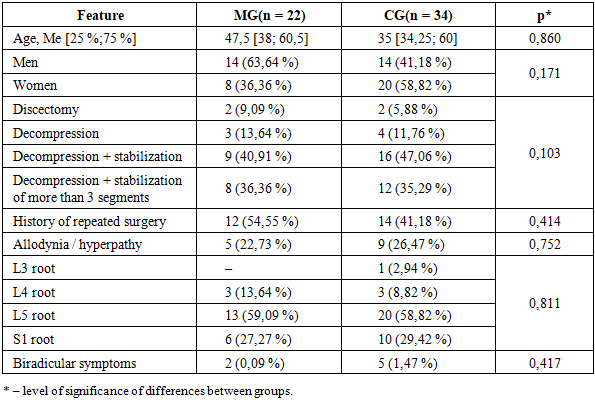
Table 1 shows the distribution of the selected groups of patients before the intervention according to the studied characteristics, no significant differences between the groups were found. For both groups, a high percentage of patients with residual radiculopathy after two or more interventions (46.6% in total), and the most frequent suffering of the L5 root should be noted (53,4%).
|
|
4. Discussion
-
According to a meta-analysis of works on FBSS [15], the incidence of radicular pain syndrome without an obvious compression substrate is 4.8-10.2% among all postoperative problems. The incidence of epidural fibrosis, according to the same study, reaches 34%, and if fibrosis is not considered as an independent factor of compression along with residual stenosis or spinal disc herniation, then the incidence of radicular pain will be even higher. The relationship between the clinical outcomes of spinal interventions and the severity of epidural fibrosis according to MRI data has not been proven at the moment, as well as the importance of methods for its prevention, therefore, the severity of the cicatricial process was not taken into account in this work. The incidence of non-compression radicular pain syndrome was 11.46% among patients with various pain syndromes and / or pathological conditions after surgery for DDD of the lumbar spine. It should be noted that at the selection stage, out of 91 patients with pain in the lower extremity, 26 were excluded based on the results of positive test blocks or other potential generators of pseudoradical pain.
The effectiveness of epidural blockade was confirmed by one randomized controlled trial [12], 59% of patients showed a positive result in the form of a 50% reduction in pain syndrome during the first year. Among the shortcomings of the study are a large number of repeated injections (on average 4 per year), the use of the least advantageous anatomical caudal approach, and the recognition of the result as positive if the effect lasts at least 3 weeks. V. Wilde et al, based on the analysis of 5 works, conclude that there is insufficient evidence of the efficacy of EB in the treatment of postoperative pain syndrome. In the present study, in the control group, satisfactory results were achieved with EB in 55.88% of patients with a single injection with an effect duration of 6 months, in 44.12% the effect persisted for a year. Positive differences may be associated with the transforaminal route of steroid administration - much closer to the zone of the alleged inflammation compared to the caudal route with a higher concentration of the drug. The value of the selectivity of administration is indirectly confirmed by the analysis of the results of the use of percutaneous adhesiolysis - an intervention with selective catheterization of the epidural space with a flexible X-ray-positive catheter and the introduction of a steroid through it in combination with hyaluronidase and hypertonic sodium chloride solutions. The procedure demonstrated to be more effective than the caudal block, but the result was more influenced by the positioning of the catheter in the ventral epidural space, rather than the use of enzymes and aggressive solutions.
The efficacy of PRF for the treatment of radicular pain has been confirmed by a randomized, double-blind, placebo-controlled trial in cervical spine pathology. In many prospective and retrospective [20] studies, rather contradictory results were obtained - the number of patients with satisfactory outcomes did not exceed 50%, there were no significant differences in the dynamics of the studied indices compared to the control group, the worst results were in patients with FBSS. It should be noted that all the mentioned studies included patients with various pathologies, including surgically significant conditions in the form of IVD hernias and degenerative stenosis, for which the ineffectiveness of conservative treatment is an expected clinical situation. The pain scale and the Oswestry index have traditionally been used to assess the results, the latter was developed primarily to measure disability in back pain, rather than radiculopathy. In a number of high-level studies comparing the results of surgery and therapy in the treatment of IVD hernias, degenerative stenosis and spondylolisthesis, there were no significant differences in these parameters between the groups after treatment, the differences were only in the SBI index, specially designed to assess radiculopathy. In the pathogenesis of radiculopathy, inflammation is recognized by all as the leading component, and the use of corticosteroids is an obvious pathogenetic component of treatment. The exclusion of the use of steroids in the selection of patients for PRF or selection based on the ineffectiveness of EB may negatively affect the expected result. The combination of EB and PRF was studied in the work of W. Koh et al. [22] and was significantly more effective than isolated EB.
Higher results (81.8% of positive results within 6 months, persistence of the effect for a year in 72.73% of patients) obtained in the study can be explained by the peculiarities of its arrangement on the basis of data obtained during literary search. Patients were included only after excluding the surgical substrate of radicular pain syndrome, with the additional exclusion of other mechanisms and sources of pain in controversial cases using test blockades.
5. Conclusions
-
Based on the results of this study, pulsed radiofrequency ablation and epidural steroid administration are effective and safe methods for the treatment of postoperative radicular pain syndrome in the absence of surgically significant compression substrates. The use of PRF in combination with EB is a more effective technique compared to isolated EB, which is confirmed by significant differences in the number of patients with satisfactory results (81.82% and 55.88%, p = 0.045), as well as a large decrease in the SBI index after the intervention, p = 0,021.